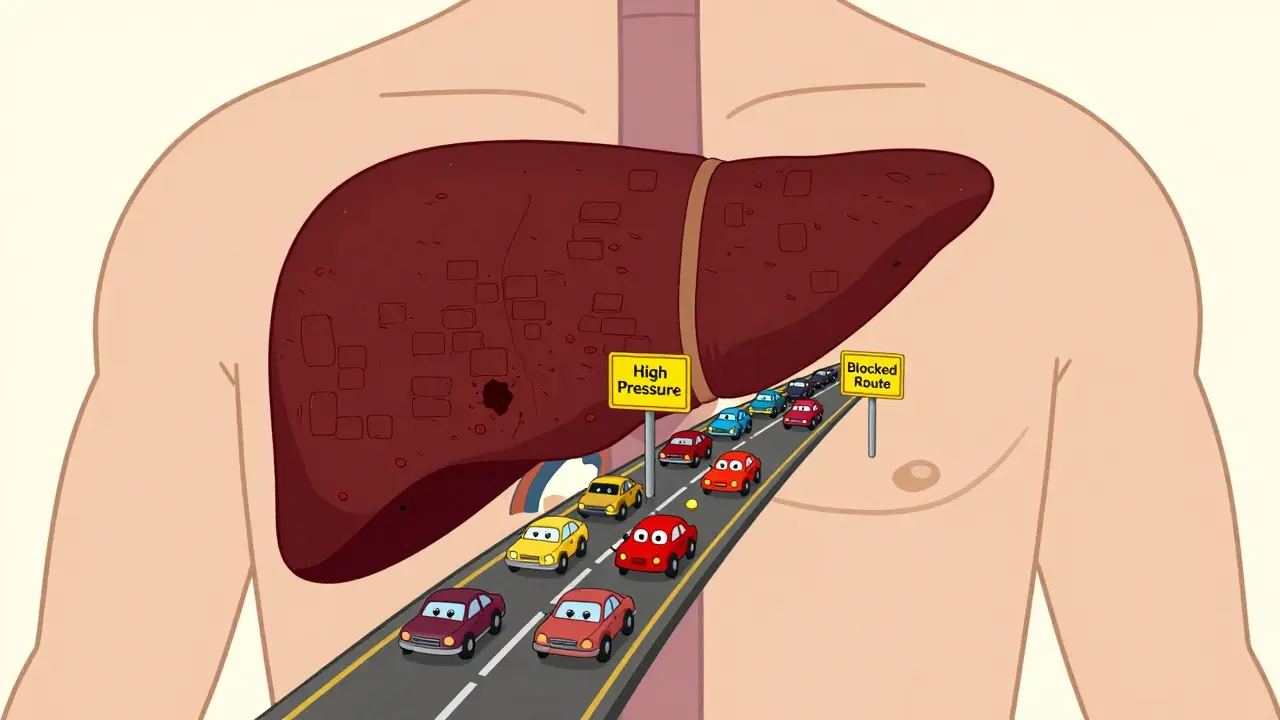
Imagine a traffic jam in your body’s most critical highway. That is essentially what Portal Hypertension is. It occurs when blood flow through the portal vein-the main vessel carrying blood from your digestive organs to your liver-is blocked or slowed down. This causes pressure to build up behind the blockage, much like water backing up in a clogged pipe.
This condition isn't just a minor inconvenience; it's a serious medical state that affects nearly everyone with advanced liver disease. According to the American Association for the Study of Liver Diseases (AASLD), about 90% of cases are caused by cirrhosis, where healthy liver tissue is replaced by scar tissue. The remaining 10% fall under non-cirrhotic portal hypertension, often due to blood clots or other rare conditions. If left unchecked, this high pressure forces blood to find alternative routes, leading to dangerous complications like swollen veins and fluid buildup in the abdomen.
Understanding the Mechanics of Portal Pressure
To understand why this happens, you need to look at the numbers. Normal pressure in the portal venous system ranges between 5 and 10 mmHg. When that pressure exceeds 10 mmHg, or specifically when the hepatic venous pressure gradient (HVPG) rises above 5 mmHg, we diagnose portal hypertension. But here is the critical threshold: an HVPG of 10 mmHg or higher is considered "clinically significant." At this level, the risk of life-threatening complications spikes dramatically.
The mechanism is twofold. First, the scarred liver creates physical resistance to blood flow. Second, the body releases chemicals like nitric oxide that cause blood vessels in the gut to widen (vasodilation). This sends even more blood toward the liver, further increasing the pressure. It’s a vicious cycle. Without intervention, about 70% of patients with cirrhosis will develop clinically significant portal hypertension within five years of their diagnosis.
Varices: The Silent Threat
One of the most feared complications is the development of esophageal varices. These are enlarged veins in the lower part of your esophagus. Because the liver is blocked, blood backs up into smaller vessels that aren't designed to handle high volume. They stretch, thin out, and can rupture.
Here is the reality check: roughly 50% of people with cirrhosis will develop these varices within ten years. For those with medium to large varices, the annual risk of bleeding is between 5% and 15%. A bleed is a medical emergency. Patients often describe vomiting liters of blood-a terrifying experience that requires immediate ICU care. The mortality rate for acute variceal bleeding remains unacceptably high, sitting at 15-20% within six weeks if not managed aggressively.
Prevention is key. Doctors use two main strategies:
- Non-selective beta-blockers (NSBBs): Medications like propranolol reduce heart rate and cardiac output, lowering portal pressure. Studies show they can reduce the risk of first-time bleeding by 45% compared to placebo.
- Endoscopic Band Ligation (EBL): During an endoscopy, doctors place small rubber bands around the varices to cut off blood supply and allow them to shrink. This method reduces rebleeding rates to 20-30%, significantly better than older sclerotherapy techniques.
Ascites: Fluid Accumulation and Quality of Life
If varices are the silent threat, ascites is the daily burden. Ascites is the accumulation of fluid in the abdominal cavity. It affects about 60% of cirrhosis patients within ten years. Imagine wearing a heavy, tight belt filled with water. That is what patients feel. It causes severe abdominal pain, shortness of breath, and makes standing for long periods impossible.
Managing ascites starts with lifestyle changes. You must restrict sodium intake to less than 2000mg per day. Most patients also take diuretics-specifically a combination of spironolactone and furosemide-to help the kidneys remove excess fluid. In uncomplicated cases, this approach works for 95% of patients.
However, when ascites becomes "refractory" (meaning it doesn't respond to medication), the situation gets complicated. About 10% of patients develop refractory ascites within two years of initial onset. Treatment then shifts to therapeutic paracentesis, where doctors drain 4-6 liters of fluid at a time using a needle. To prevent shock from rapid fluid loss, albumin is infused intravenously during the procedure. While effective, frequent taps take a toll on patients' quality of life, with many reporting scores 35-40 points lower on health metrics compared to healthy peers.
Advanced Interventions: TIPS and Beyond
When medications and simple procedures fail, doctors turn to the Transjugular Intrahepatic Portosystemic Shunt (TIPS). This is a major interventional radiology procedure. A specialist creates a new channel (shunt) inside the liver connecting the portal vein to the hepatic vein. This bypasses the scarred tissue, instantly dropping portal pressure.
TIPS has a technical success rate of 90-95%, and 78% of patients report significant improvement in ascites control. However, it comes with trade-offs. By diverting blood away from the liver, toxins that the liver usually filters can enter the bloodstream, leading to hepatic encephalopathy (confusion and brain fog). Up to 30% of patients develop this side effect within a year. Therefore, TIPS is reserved for severe cases where the benefits outweigh the cognitive risks.
| Strategy | Primary Use | Effectiveness | Key Risks/Side Effects |
|---|---|---|---|
| Non-Selective Beta-Blockers | Prevent first bleed | Reduces risk by 45% | Fatigue, low blood pressure, dizziness |
| Endoscopic Band Ligation | Treat existing varices | Reduces rebleeding to 20-30% | Post-band ulceration, dysphagia |
| Diuretics + Sodium Restriction | Control mild-moderate ascites | Effective in 95% of uncomplicated cases | Electrolyte imbalance, kidney strain |
| TIPS Procedure | Refractory ascites / recurrent bleeding | 90-95% technical success | Hepatic encephalopathy (20-30%) |
Emerging Treatments and Diagnostic Tools
The landscape of liver care is evolving rapidly. For decades, measuring HVPG required invasive catheterization. Now, non-invasive markers are gaining ground. Spleen stiffness measurement via elastography (like FibroScan) approaches 85% accuracy in predicting clinically significant portal hypertension. This could spare many patients from invasive tests.
In therapeutics, new drugs are entering the pipeline. Simtuzumab, a monoclonal antibody targeting lysyl oxidase-like 2 (LOXL2), received FDA breakthrough designation in late 2023 for non-cirrhotic portal hypertension. Early trials showed a 35% reduction in portal pressure. Additionally, AI algorithms are being trained to predict variceal bleeding with over 90% accuracy, allowing for earlier, targeted interventions.
Despite these advances, the root cause-rising rates of NAFLD (Non-Alcoholic Fatty Liver Disease)-remains a challenge. NAFLD now accounts for 24% of global cirrhosis cases, up from 15% in 2015. As obesity and metabolic syndrome increase, so does the burden of portal hypertension, making early detection and lifestyle management more critical than ever.
What is the difference between portal hypertension and systemic hypertension?
Systemic hypertension refers to high blood pressure in the main arteries supplying the body, measured by a standard cuff. Portal hypertension is high pressure specifically within the portal vein system that carries blood to the liver. You can have normal blood pressure but still suffer from severe portal hypertension due to liver scarring.
Can portal hypertension be cured?
Currently, there is no cure for portal hypertension itself. Treatment focuses on managing complications like varices and ascites. The only definitive cure for the underlying cause (usually cirrhosis) is liver transplantation. New drugs aim to reduce pressure, but they do not reverse established scarring.
How much salt should I eat if I have ascites?
Patients with ascites are typically advised to restrict sodium intake to less than 2000mg (2 grams) per day. This helps prevent fluid retention. Avoid processed foods, canned soups, and fast food, as these are hidden sources of excessive salt.
What are the signs of a variceal bleed?
The most obvious sign is vomiting bright red blood or material that looks like coffee grounds. Other signs include black, tarry stools (melena), dizziness, fainting, or confusion. If you experience any of these, seek emergency medical attention immediately.
Is TIPS a permanent solution?
TIPS provides long-term relief for many, but the shunt can narrow over time (stenosis) or become blocked. Regular follow-up ultrasounds are needed to ensure patency. Some patients may require revision procedures or eventual liver transplantation if liver function continues to decline.