Kidney Function Dose Calculator
How Your Kidneys Affect Medication Safety
Your kidney function determines how quickly your body clears medications. Poor kidney function can lead to dangerous drug buildup.
Clinical Note This tool estimates kidney function to guide dose adjustments for medications like vancomycin, antibiotics, and blood pressure drugs.
Ever wonder why a pill that works perfectly for your friend gives you a headache? It’s not just luck or coincidence. It’s your body’s unique way of handling the drug - and that’s called pharmacokinetics. This isn’t some abstract science term. It’s the real reason some people get sick from a dose that’s safe for others. Understanding how your body absorbs, distributes, metabolizes, and gets rid of drugs isn’t just for doctors. It’s the key to knowing why side effects happen - and how to avoid them.
What Happens When You Swallow a Pill?
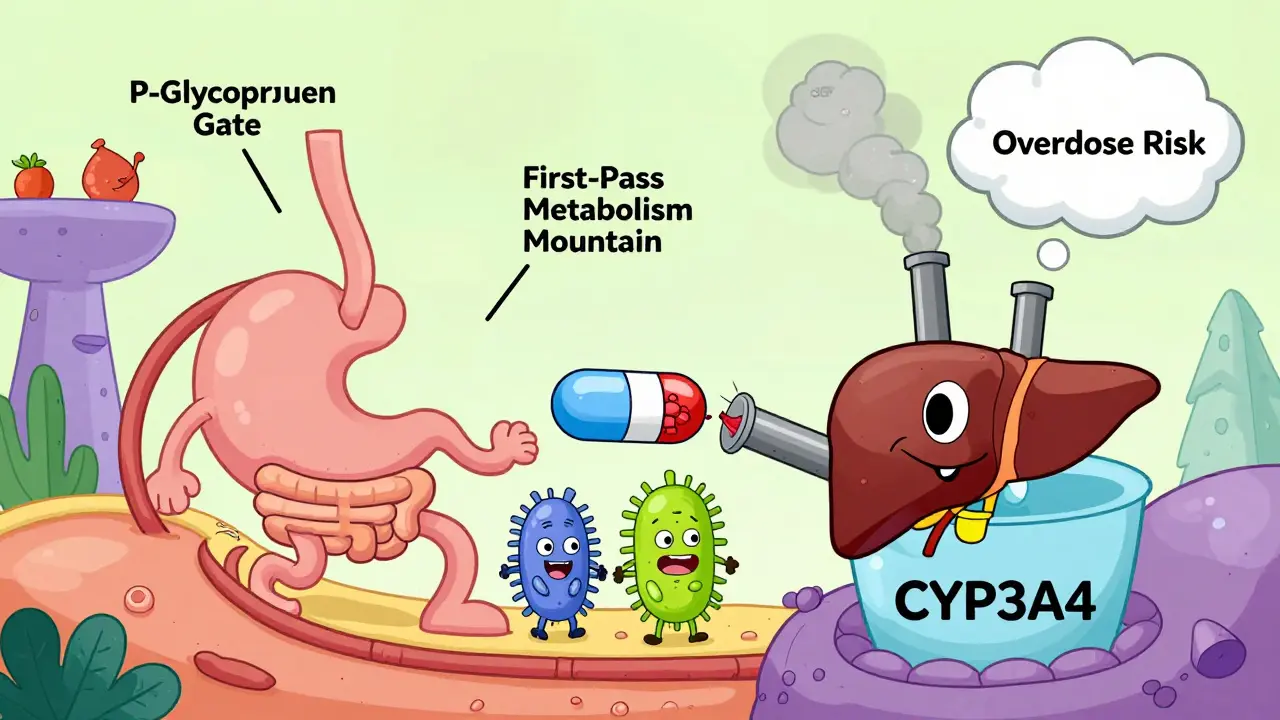
Let’s say you take an ibuprofen tablet. It doesn’t just dissolve and magically fix your headache. First, it has to get into your bloodstream. That’s absorption. Most drugs, like ibuprofen, pass through your stomach and intestines by passive diffusion. About 95% of all drugs use this method. But your gut’s pH, how fast food moves through you, and even certain proteins like P-glycoprotein can block or slow absorption. For example, if you’re on digoxin for heart issues, P-glycoprotein can cut its absorption by up to 70%. That means you might need a higher dose - or a different drug - if your body’s transporters are extra active.Not all drugs are swallowed. Some are injected, inhaled, or applied to the skin. Each route changes how much of the drug actually reaches your blood. IV drugs give you 100% of the dose because they go straight in. Oral drugs? Usually only 40-60%. Why? Because your liver breaks down part of it before it even gets to your bloodstream. That’s called first-pass metabolism. And it’s why some drugs, like nitroglycerin, are given under the tongue - to skip the liver entirely.
Where Does the Drug Go After It Enters Your Blood?
Once in your bloodstream, the drug doesn’t just sit there. It gets pulled into tissues - muscles, fat, brain, even bones. How far it spreads depends on something called volume of distribution (Vd). A low Vd (0.1-0.3 L/kg) means the drug stays mostly in your blood. A high Vd (>1.0 L/kg) means it’s soaked into your tissues. Lithium, for example, has a high Vd. That’s why it takes days to reach steady levels - and why missing a dose can throw off your mood control.Another big player? Protein binding. About 98% of warfarin, the blood thinner, sticks to albumin in your blood. Only the 2% that’s free can work. If another drug - say, an antibiotic - kicks warfarin off those proteins, suddenly you’ve got way more active drug in your system. That’s why people on warfarin can bleed easily after starting a new medicine. It’s not the antibiotic’s fault. It’s the pharmacokinetic ripple effect.
Your Liver: The Drug’s Main Processing Plant
Your liver doesn’t just filter toxins. It transforms drugs into forms your body can flush out. This happens mostly through enzymes called Cytochrome P450 (CYP). CYP3A4 alone handles half of all prescription drugs. But here’s the catch: these enzymes vary wildly from person to person.Genetics play a huge role. About 3-10% of Caucasians have a version of CYP2D6 that barely works. That means codeine - which needs to be turned into morphine by this enzyme - gives them no pain relief. Meanwhile, super-metabolizers might turn codeine into morphine too fast, risking overdose. Same pill. Different bodies. Different outcomes.
Age matters too. After 65, liver blood flow drops 30-50%. That slows metabolism. Benzodiazepines like diazepam can hang around for 100 hours in older adults, instead of the usual 20-50. That’s why elderly patients get dizzy, fall, or pass out on doses that are fine for younger people.
How Your Kidneys Clean Up the Mess
Most drugs leave your body through your kidneys. Your glomerular filtration rate (GFR) tells you how fast that happens. Normal GFR? 90-120 mL/min. If you have kidney disease, that number can drop below 15. That’s a red flag. Vancomycin, an antibiotic, is cleared almost entirely by the kidneys. If your doctor doesn’t adjust the dose for low GFR, you can build up toxic levels. One Reddit user, a pharmacist, shared a case where a 78-year-old patient’s creatinine jumped from 1.2 to 3.4 mg/dL - a sign of kidney damage - because their vancomycin dose wasn’t reduced for declining kidney function.Drugs like lithium and digoxin have narrow therapeutic windows. Too little? No effect. Too much? Toxicity. That’s why doctors check blood levels. But even then, timing matters. If your blood is drawn too early or too late before your next dose, the numbers lie. Studies show over 20% of hospital labs collect samples at the wrong time. That’s not just a mistake. It’s a safety risk.
Why Some Side Effects Show Up Days Later
You might think side effects happen right away. Not always. Take diazepam (Valium). It breaks down into desmethyldiazepam - a metabolite with a 100-hour half-life. That means even after you stop taking it, the active substance keeps circulating. Elderly patients on long-term benzodiazepines often feel foggy for days. It’s not the original drug. It’s the leftover metabolite.Drug interactions are another silent killer. Clarithromycin (an antibiotic) blocks CYP3A4. If you’re also taking simvastatin (a cholesterol drug), your simvastatin levels can spike 10-fold. That raises your risk of rhabdomyolysis - a muscle-destroying condition - from 0.04% to 0.5%. That’s a 12-fold increase in risk. And it’s entirely due to pharmacokinetics, not the drugs themselves.
Personalized Dosing Is Here - And It’s Changing Everything
We used to treat everyone the same. Now we know that’s dangerous. Genetic testing is already required for 28 drugs. Abacavir? Screen for HLA-B*5701. If you have it, you can’t take this HIV drug - it could kill you. Clopidogrel? Test for CYP2C19. Poor metabolizers don’t convert it to its active form. They’re at higher risk of stent clots. Testing prevents that.AI is stepping in too. DoseMeRx, an FDA-cleared tool, uses your age, weight, kidney function, and genetics to predict the right dose. In trials, it cut vancomycin dosing errors by 62%. That’s not a small win. It’s life-saving.
And the science is still evolving. New research shows gut bacteria metabolize 15-20% of oral drugs. That’s why two people with identical genes can respond differently - their microbiomes are different. The NIH just launched a $185 million project to fix the fact that 85% of pharmacokinetic studies use young, white men. That’s not science. That’s bias. And it’s costing lives.
What You Can Do
You don’t need to be a pharmacist to protect yourself. Here’s what helps:- Always tell your doctor about every supplement, herb, or OTC drug you take. Even garlic or St. John’s wort can interfere.
- Ask: “Could this drug affect my kidneys or liver?” Especially if you’re over 65 or have chronic disease.
- If you’re on blood thinners, anticonvulsants, or antibiotics, ask about therapeutic drug monitoring. It’s not optional - it’s essential.
- Don’t assume a dose is safe just because it’s the same as someone else’s. Your body isn’t theirs.
Pharmacokinetics isn’t about complex math or lab reports. It’s about your body’s unique chemistry. When you understand it, you stop seeing side effects as random bad luck. You see them as predictable - and preventable.
What does pharmacokinetics mean?
Pharmacokinetics is what your body does to a drug. It covers four steps: absorption (how it enters your bloodstream), distribution (where it goes in your body), metabolism (how your liver breaks it down), and excretion (how it leaves your body). This is different from pharmacodynamics, which is what the drug does to your body - like how it relieves pain or lowers blood pressure.
Why do some people have worse side effects than others?
It comes down to differences in absorption, metabolism, and elimination. Genetics can make your liver break down drugs too fast or too slow. Age, kidney function, liver disease, and other medications can change how much drug stays in your system. For example, a 70-year-old with reduced kidney function may have twice the drug concentration in their blood compared to a healthy 30-year-old on the same dose.
Can diet affect how a drug works?
Yes. Grapefruit juice blocks CYP3A4, which can cause dangerous spikes in drugs like statins or blood pressure meds. High-fiber meals can slow absorption of some drugs, while fatty meals can help others absorb better. Even coffee can interfere with certain antibiotics. What you eat matters more than most people realize.
Do over-the-counter drugs have pharmacokinetic risks?
Absolutely. Acetaminophen (Tylenol) is safe at 3,250 mg/day for most people - but if you drink alcohol regularly or have liver disease, your body can’t process it well. That’s when you risk liver failure. NSAIDs like ibuprofen can raise blood pressure or harm kidneys in older adults. OTC doesn’t mean harmless.
Is pharmacokinetic testing available to the public?
Some genetic tests are already offered directly to consumers - like 23andMe’s report on CYP2C19 or CYP2D6 variants. But full pharmacokinetic profiling - including liver and kidney function, protein binding, and drug interactions - is still mostly done in hospitals or specialty clinics. If you’re on multiple medications, ask your pharmacist or doctor if therapeutic drug monitoring or pharmacogenetic testing could help you.
Zola Parker
So let me get this straight - your body’s just a magic box that sometimes says 'nope' to pills? 🤔 I swear, if my liver had a Yelp page, it’d be 1 star with a review that says 'overworked, underappreciated, and definitely drunk on my wine.'
winnipeg whitegloves
This is the kind of post that makes me wanna hug a pharmacist. Seriously. I never realized how much my body’s a tiny, chaotic symphony of enzymes, transporters, and gut bacteria all arguing over who gets to process my Advil. One guy’s CYP3A4 is a VIP bouncer - another’s is a drunk intern. We’re all just walking pharmacokinetic experiments. 🙌
James Moreau
I appreciate how this breaks it down without jargon. My dad’s on warfarin and I finally get why his dose keeps changing. It’s not that he’s 'non-compliant' - it’s that his liver’s got a different playlist than the textbook. We need more of this kind of clarity in patient education. Thanks for the deep dive.
J. Murphy
so like... your liver is just a filter? and if u r old or drunk or ate grapefruit u just... explode? idk man. this is why i dont take meds unless i have to. p.s. i think the word 'pharmacokinetics' is just a scam to make doctors sound smart.
Jesse Hall
I’ve been on antidepressants for 8 years and this post made me cry. Not because I’m sad - because I finally get why some pills felt like they were working and others felt like I was just swallowing chalk. Your body isn’t broken. It’s just different. And that’s okay. 💙
Seth Eugenne
I work in a clinic and I’ve seen so many people get blamed for 'not responding' to meds. It’s not them - it’s that their liver metabolizes codeine like a caffeinated squirrel. We need to stop treating bodies like they’re all the same model. This isn’t a one-size-fits-all world. It’s a 37-variant puzzle. And we’re just starting to see the pieces. 🙏
Alex Arcilla
So let me get this straight - 85% of drug studies are done on white dudes in their 20s? And we’re shocked when grandma from Detroit has a stroke on a 'safe' dose? Bro. That’s not science. That’s a crime. And the NIH’s $185M project? It’s about damn time. I’m tired of being a guinea pig for someone else’s textbook.
Brandon Shatley
i didnt know grapefruit could mess with meds. now im scared to eat breakfast. also i think my dog might be a better metabolizer than me. he eats everything and never gets sick. maybe we should test pets instead. just sayin.